
Tennessee Is Turning Care for Sick Immigrant Children Into an Immigration Trap
About 400 medically fragile immigrant children were told continued care could trigger reporting to a Tennessee immigration office.

Gov. Bill Lee’s administration is attaching an immigration reporting threat to a medical program used by sick and disabled children.
Families whose children rely on Tennessee’s Children’s Special Services program were told last week that if the program continues paying for care after June 30, their child’s information may be shared with the Tennessee Department of Safety and Homeland Security, according to Tennessee Lookout reporting. The department houses the state’s Centralized Immigration Enforcement Division, which works with Immigration and Customs Enforcement.
The notice reached about 400 families whose children do not have permanent legal status. Many of those children are medically fragile. Some rely on feeding tubes, ventilators, metabolic formula, medications, specialists, therapy, and other supports that cannot be replaced by a last-minute handoff or a trip to the emergency room.
The choice placed before families is not really a choice: continue care and risk exposure to immigration enforcement, or leave the program and risk losing the medical support that keeps a child stable.
Children’s Special Services is a decades-old public program for children with disabilities, chronic illnesses, and, in some cases, terminal diagnoses. It serves uninsured and underinsured children across Tennessee and helps pay for care that families often cannot obtain on their own, including hospitalizations, specialists, therapists, medications, medical supplies, social workers, and in-home support.
More than 4,600 children are enrolled statewide. The reporting threat targets a smaller group of immigrant children without permanent legal status, but the harm is not abstract. It lands on families already managing complex medical needs and already living with the fear that contact with government systems can expose them to immigration enforcement.
That is what makes Tennessee’s decision so dangerous. The state is not simply changing paperwork. It is attaching immigration fear to pediatric medical care.
Among the families affected is Gabriella’s. Tennessee Lookout identified her only by her first name because she fears her family could be targeted by immigration officials for speaking publicly. Her family has a pending asylum claim.
Her 10-year-old son has complex medical conditions, including spina bifida, autism, and kidney disease. He uses a wheelchair and has relied on Children’s Special Services for seven years.
After receiving the state’s notice, Gabriella and her husband decided to withdraw him from the program.
The decision came from fear. Fear that continuing care could expose the family to immigration officials. Fear that detention would interrupt her son’s care. Fear that the system asking for information about her child could become the system that separates him from the people keeping him alive.
“I don’t want immigration to come to my house,” Gabriella told the Tennessee Lookout. “I don’t want them to put us in detention. In detention, my son wouldn’t get any care.”
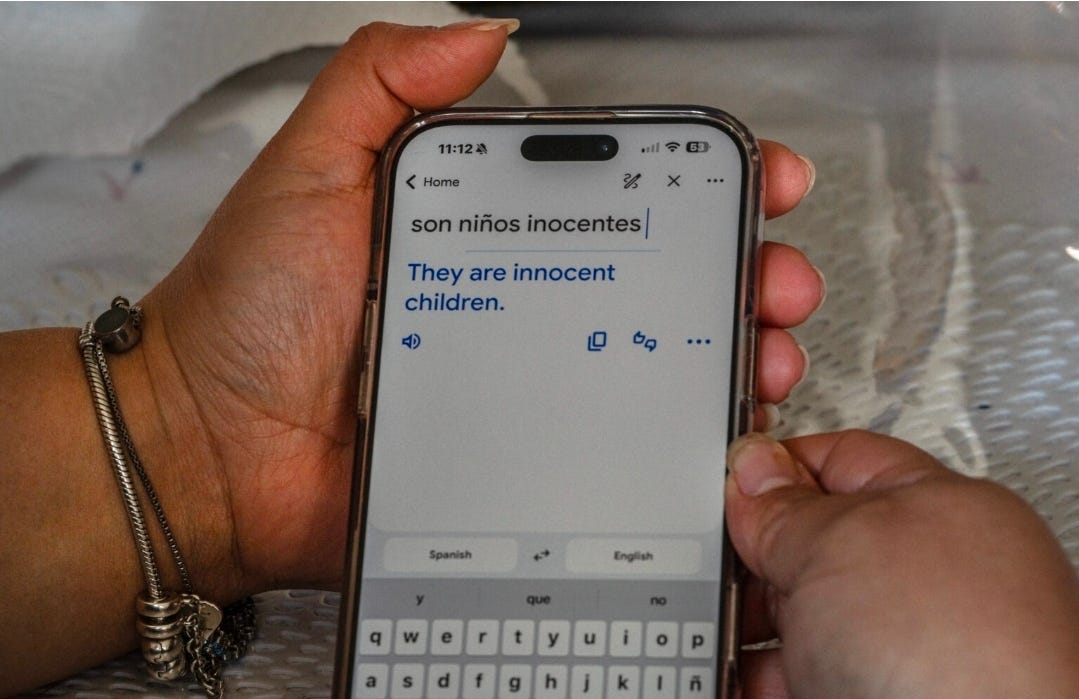
She later used a translation app to explain what she wanted people to understand.
“They are innocent children,” the translation read.
That sentence is the center of this story. The children affected by Tennessee’s decision are not immigration policy talking points. They are children with kidney disease, cancer treatment, disabilities, feeding tubes, ventilators, therapies, braces, catheters, medications, and parents trying to keep them safe.

The state’s notice cited a new Tennessee law that the Department of Health says requires reporting immigrants seeking or receiving public benefits who do not have legal permanent status. Legal advocates for low-income patients dispute that interpretation and say the law applies only to adults.
That dispute matters because the state’s interpretation is already changing family decisions. The Tennessee Justice Center, a nonprofit legal advocacy firm, has been searching for plaintiffs willing to join a legal challenge. As of Friday, according to Tennessee Lookout, the group had not found a family willing to join.
Michele Johnson, the organization’s executive director, said families are scared. Even if parents are not fully identified in public court filings, their identities would have to be shared with lawyers defending the state during litigation.
That is how enforcement pressure works even before a raid, detention, or deportation order. It can make families afraid to seek help, afraid to challenge the state, and forced to weigh a child’s medical stability against the possibility that a government form could expose them to immigration enforcement.
Public health workers and providers are now trying to prevent children from losing care. Dr. Morgan McDonald, who sits on Nashville’s Metro Health Board, described nurses scrambling for ventilators, feeding tubes, metabolic formula, and other supports to keep children out of the hospital and alive.
Public health staff have been working around the clock, she said, but the resources available to families are shrinking.
That scramble is the consequence of Tennessee’s decision. A child who needed care last week still needs care this week. Feeding tubes, catheters, braces, medications, specialists, and infection-prevention care do not become optional because the state attached immigration reporting to the program.
The Republican sponsor who defended the health department’s interpretation pointed to emergency rooms as an alternative, saying federal protections for emergency and lifesaving medical services remain in place.
That answer collapses when placed next to the actual needs of the children in this program.
Emergency rooms may treat emergencies. They do not replace ongoing specialty care. They do not replace feeding tube supplies, ventilator support, metabolic formula, kidney medications, catheters, annual leg braces, physical therapy, in-home care, social workers, or the care coordination that keeps medically fragile children stable before a crisis becomes an emergency.
Gabriella made that point plainly. Her son needs therapies and doctors the family cannot afford. Emergency rooms do not provide the ongoing supports stacked inside his bedroom: catheters, gloves, diapers, kidney medication, infection prevention medication, leg braces, and equipment to help lift him out of bed.
“My husband pays taxes,” she told Tennessee Lookout. “We are not trying to take anything from other people. We are just trying to help our son, as any parent would.”
That is the reality Tennessee’s policy is pressuring families to abandon.
The Tennessee Department of Health did not respond to repeated requests for information from Tennessee Lookout last week. State Sen. Heidi Campbell, a Nashville Democrat, said the department also stopped answering her questions, citing potential litigation.
Campbell said lawmakers have a right and obligation to know whether state agencies are operating within their authority, especially when 400 seriously ill children may have been swept into immigration reporting beyond what the law requires.
The lack of answers adds another layer of harm. Families are being forced to make urgent medical decisions while the state refuses to fully explain how it is applying the law, what information will be shared, when it will be shared, and what protections, if any, exist for children who depend on the program.
That uncertainty is not separate from the policy. It is part of the pressure.
For families already afraid of immigration enforcement, the line between a health department notice and an enforcement threat is not theoretical. Gabriella said that since immigration sweeps in Nashville detained more than 100 people, she and her husband usually drive separately so their children do not lose both parents if one of them is detained. They travel together only to church on Sundays.
Each day, when her husband leaves for work, they embrace and pray for his safe return.
That is the atmosphere Tennessee is placing around a children’s medical program. Not a neutral benefits update. Not ordinary verification. A reporting threat delivered to families whose children need care.
Immigration enforcement does not have to enter a home to change how a family lives. It can shape how parents drive, how they respond to letters, whether they keep appointments, whether they seek legal help, and whether they trust public health systems designed to keep children alive.
Tennessee’s policy shows how state enforcement infrastructure can reach medically fragile children through a health department envelope.
It also shows how immigration fear can make families disappear from care before the state ever has to formally remove them. Families can withdraw from the program before any formal enforcement action occurs. Children can lose support, nurses and social workers can be left scrambling, and hospitals can become the fallback for problems that could have been prevented.
For the families affected, the deadline is not an administrative date. It is a medical cliff.
June 30 is the point at which parents must decide whether to keep accepting help through Children’s Special Services knowing the state says information may be reported to an immigration enforcement office. For a child in the middle of chemotherapy, dependent on a feeding tube, using a ventilator, or living with a complex disability, that kind of deadline can destabilize an entire care plan.
The state created that pressure. Tennessee officials chose to apply the reporting requirement to a children’s medical program, sent the notice, and placed the burden on families already caring for some of the sickest children in the state.
The children did not create this crisis. They are the ones being made to carry it.
Immigration enforcement does not only happen when agents knock on doors or stop people in the street.
It can move through health departments, benefit offices, reporting rules, forms, databases, and deadlines that force families to choose between the care their children need and the fear of being exposed to immigration authorities.
Tennessee’s policy shows how enforcement pressure can reach a medically fragile child without an ICE agent ever entering the room. A program built to help sick and disabled children stay stable can become another place where immigrant families are made to feel unsafe.
Americans Against ICE documents these systems because the harm is not limited to raids. It reaches hospitals, schools, county offices, detention networks, public benefits, family homes, and the care systems people depend on to survive.
Support this work by upgrading to a paid subscription.